Facts about Botulism

Infant botulism (first recognized in 1976) is the most common form of the ailment in the United States, but is rarely diagnosed in other countries.

Classic symptoms of food-borne botulism occur 12–36 hours after consuming the botulinum toxin, although they can occur as early as 6 hours or as late as 10 days.

One study showed that approximately 5 percent of children whose death was attributed to Sudden Infant Death Syndrome had actually died of botulism.

Outbreaks of foodborne botulism involving two or more persons occur during most years and usually are caused by eating contaminated home-canned foods.



The respiratory failure and paralysis that occur with severe botulism may require a patient to be on a breathing machine for weeks, plus intensive medical and nursing care.

Like the other forms of botulism, the symptoms are caused by the absorption of botulinum toxin, and typically progress to a symmetric descending, flaccid paralysis.
Tests used in diagnosing botulism may include a brain scan, cerebrospinal fluid examination, nerve conduction test (electromyography, or EMG), and an Edrophonium Chloride (Tensilon) test for myasthenia gravis.
Typical instances of botulism would be home-bottled preserves used in salads.

Cases of inadvertent botulism have occurred due to overdose or accidental intravenous injection of Botox, which is a commercially producted from botulinum toxin.

Between 1910 and 1919, the death rate from botulism was 70 percent in the United States.

The case fatality rate is less than 1 percent for hospitalized infants with botulism.


Foodborne botulism has more frequently been from home-canned foods with low acid content, such as carrot juice, asparagus, green beans, beets, and corn.

Wound botulism can be prevented by promptly seeking medical care for infected wounds, and by avoiding punctures by unsterile implements such as needles used for street drug injections.

Death rates from botulism dropped to 9 percent in the 1980s, and 2 percent in the early 1990s, mainly because of the development of artificial respirators.

Nevertheless, the majority of infants with botulism have no history of ingestion of honey, and the exact source of the offending spores is unclear about 85 percent of the time.

Foodborne botulism can be especially dangerous as a public health problem because many people can be poisoned from a single contaminated food source.

Canned foods may also indicate botulism infestation by outward bulges in the can, which result from gas production (perhaps during bacterial growth) causing increased pressure inside the can.

A patient with severe botulism may require a breathing machine (ventilator) as well as intensive medical and nursing care for several months.

Physicians may consider the diagnosis if the patient's history and physical examination suggest botulism.
Patients who survive an episode of botulism poisoning may have fatigue and shortness of breath for years and long-term therapy may be needed to aid their recovery.

The number of cases of foodborne and infant botulism has changed little in recent years, but wound botulism has increased because of the use of the illegal drug, black tar heroin (Passaro et al.

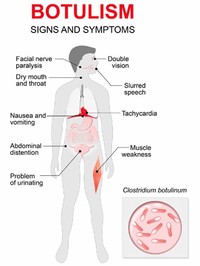
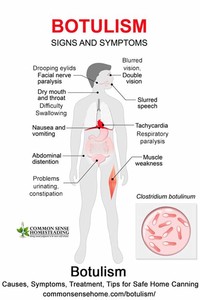
Clostridium botulinum is the bacterium that produces the toxin botulin, the causative agent in botulism (Ryan and Ray 2004).

Good supportive care in a hospital is the mainstay of therapy for all forms of botulism.

Of these, approximately 25 percent are foodborne, 72 percent are infant botulism, and 3 percent are wound botulism.

Botulism (from the Latin word botulus, meaning sausage) is a rare, but serious paralytic illness caused by a nerve toxin, botulin, that is produced by the bacterium Clostridium botulinum.
Other diseases, such as Guillain-Barrй syndrome, stroke, and myasthenia gravis, can appear similar to botulism, and special tests may be needed to exclude these other conditions.
