Facts about Hepatitis


Five percent of patients do not clear the infection and develop chronic infection; only these people are at risk of long term complications of hepatitis B.

Alcoholic hepatitis can vary from mild, with only liver test elevation, to severe liver inflammation, with development of jaundice, prolonged prothrombin time, and liver failure.

Hepatitis B is endemic in a number of (mainly South-East Asian) countries, making cirrhosis and hepatocellular carcinoma big killers.

See below for non-alcoholic steatohepatitis (NASH), effectively a consequence of metabolic syndrome.

Hepatitis A can be spread through personal contact, consumption of raw sea food, or drinking contaminated water.

Statins can cause elevations of liver function blood tests normally without indicating an underlying hepatitis.

Certain liver function tests, which mostly measure liver enzymes in the blood, indicate the diagnosis of hepatitis.

Another type of hepatitis, hepatitis G, has been identified, and is probably spread by blood and sexual contact.

Lastly, human variability is such that any drug can be a cause of hepatitis.

Alcoholic hepatitis is characterized by a variable constellation of symptoms, which may include feeling unwell, enlargement of the liver, development of fluid in the abdomen (ascites), and modest elevation of liver blood enzymes.

Usually alcoholic hepatitis comes after a period of increased alcohol consumption.

The diagnosis of autoimmune hepatitis is best achieved with a combination of clinical and laboratory findings.

Patients who drink alcohol to excess are also more often than others found to have hepatitis C. The combination of hepatitis C and alcohol consumption accelerates the development of cirrhosis in Western countries.
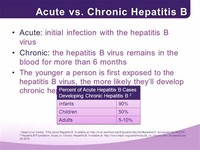
Chronic hepatitis develops in the 15 percent of patients who are unable to eliminate the virus after an initial infection.
The patient's immune system makes antibodies against hepatitis A that confer immunity against future infection.

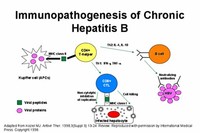
Patients with chronic hepatitis B have antibodies against hepatitis B, but these antibodies are not enough to clear the infection that establishes itself in the DNA of the affected liver cells.

Infected persons begin excreting the hepatitis A virus with their stool two weeks after the appearance of the first symptoms.


Anomalous presentation of human leukocyte antigen (HLA) class II on the surface of hepatocytes—possibly due to genetic predisposition or acute liver infection—causes a cell-mediated immune response against the body's own liver, resulting in autoimmune hepatitis.

Autoimmune hepatitis has an incidence of 1-2 per 100,000 per year, and a prevalence of 15-20/100,000.

Some drugs on the market, such as certain anti-diabetic and antiretroviral drugs, have been connected to incidences of hepatitis as well.

Hepatitis A causes an acute form of hepatitis that does not have a chronic stage, and carries a 1 percent risk of developing into fulminant hepatitis.

Hepatitis E produces symptoms similar to hepatitis A (also transmitted by the feco-oral route), although it can take a fulminant course in some patients, particularly pregnant women; it is more prevalent on the Indian subcontinent.
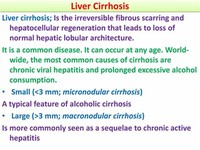
Cirrhosis can also occur upon repeated attacks of hepatitis, as most commonly seen in the form of alcoholic hepatitis.

Hepatitis B is caused by a hepadnavirus (virus family Hepadnaviridae, having partially double-stranded, partially single stranded non-circular DNA).

Ethanol, mostly in alcoholic beverages, is an important cause of hepatitis.

People with hepatitis A are advised to rest, stay hydrated, and avoid alcohol.

Hepatitis A, or infectious jaundice, is caused by a picornovirus (RNA virus).

The clinical course of drug-induced hepatitis is quite variable, depending on the drug and the patient's tendency to react to the drug.
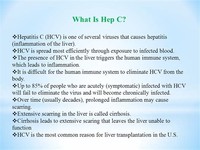
Hepatitis C (originally "non-A non-B hepatitis") can be transmitted through contact with blood (major cause of transfusion related hepatitis), sexual contact (much lower than with hepatitis B), as well as in utero.

Hepatitis B infections result in 500,000 to 1,200,000 deaths per year worldwide due to the complications of chronic hepatitis, cirrhosis, and hepatocellular carcinoma.

The anti-diabetic drug troglitazone was withdrawn in 2000 for causing hepatitis.

Hepatitis C may lead to a chronic form of hepatitis, culminating in cirrhosis.
An inactivated vaccine is available that will prevent infection from hepatitis A for life and is indicated for those planning to travel to endemic areas as well as those with chronic liver disease.

Hepatitis D is an RNA virus that can only exist is the presence of Hepatitis B infection, whether there is superinfection or coinfection.

NASH is becoming recognized as the most important cause of liver disease second only to Hepatitis C in numbers of patients going on to cirrhosis.