Facts about Insulin

Confusingly, the primary sequence of proinsulin goes in the order "B-C-A," since B and A chains were identified on the basis of mass, and the C peptide was discovered after the others.

Increased blood glucose levels after a meal is a stimulus for prompt release of insulin from the pancreas.


Non-diabetics' beta cells routinely and automatically manage this by continual glucose level monitoring and insulin release.

The use/abuse of exogenous insulin is widespread among the bodybuilding community.

Insulin is an anabolic (part of metabolism that builds larger molecules) polypeptide hormone and regulates carbohydrate metabolism in animals.

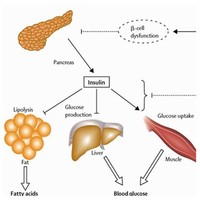
Two types of tissues are most strongly influenced by insulin, as far as the stimulation of glucose uptake is concerned: muscle cells (myocytes) and fat cells (adipocytes).

On the other hand, if too little insulin is delivered, there will be hyperglycemia.

Most insulins used clinically today are produced this way, as they are less likely to produce an allergic reaction.

Insulin-dependent diabetics require a base level of insulin (basal insulin), as well as short-acting insulin to cover meals (bolus insulin).

The patent for insulin was sold to the University of Toronto for one dollar.

The increased insulin level causes glucose absorption and storage in cells, reducing glycogen to glucose conversion, reducing blood glucose levels, and so reducing insulin release.

The central problem for those requiring external insulin is picking the right dose of insulin and the right timing.

The insulin administration aspect remains experimental, but the blood glucose test aspect of "wrist appliances" is commercially available.

Currently, inhaled insulin is short acting and is typically taken before meals; an injection of long-acting insulin at night is often still required (NICE 2006).
Advantages to the patient are better control over background or "basal" insulin dose, bolus doses calculated to fractions of a unit, and calculators in the pump that help with dosing "bolus" infusions.

Bovine insulin differs from human in only three amino acid residues, and porcine insulin in one.


The word insulin comes from the Latin insula, meaning "island," as it is produced in mammals in the Islets of Langerhans in the pancreas.

Researchers have produced a watch-like device that tests for blood glucose levels through the skin and administers corrective doses of insulin through pores in the skin.

Unity in nature is seen in the fact that insulin's structure varies slightly between species of animals, and is particularly close among vertebrates.
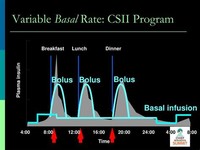
Maintaining the basal rate and the bolus rate is a continuous balancing act that insulin-dependent diabetics have to manage each day.

On July 23, 2004, news reports claimed that a former spouse of a prominent international track athlete said that, among other drugs, the ex-spouse had used insulin as a way of "energizing" the body.



Clinical insulins are specially prepared mixtures of insulin plus other substances.

Instead insulin is usually taken as subcutaneous injections by single-use syringes with needles, an insulin pump, or by repeated-use insulin pens with needles.

The initial sources of insulin for clinical use in humans were cattle, horse, pig, or fish pancreases.

Another "improvement" would be a transplantation of the pancreas or beta cell to avoid periodic insulin administration.

Nearly half of those who got an islet cell transplant are insulin-free one year after the operation; by the end of the second year that number drops to about one in seven.


Patients with type 2 diabetes mellitus have insulin resistance or relatively low insulin production, or both; some type 2 diabetics eventually require insulin when other medications become insufficient in controlling blood glucose levels.
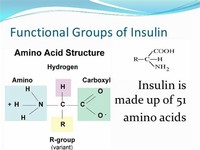
Insulin is composed of 51 amino acid residues (constituents) in total and has a molecular weight of 5808 Da.

Differences in suitability of beef, pork, or fish derived insulin for individual patients have been primarily due to low preparation purity resulting in allergic reactions to the presence of non-insulin substances.

Release of insulin is strongly inhibited by the stress hormone norepinephrine (noradrenaline), which leads to increased blood glucose levels during stress.



Activation of insulin receptors leads to internal cellular mechanisms, which directly affect glucose uptake by regulating the number and operation of protein molecules in the cell membrane which transport glucose into the cell.

Like nearly all other proteins introduced into the gastrointestinal tract, it is reduced to fragments (even single amino acid components), whereupon all "insulin activity" is lost.

The amount of insulin in circulation has extremely widespread effects throughout the body.

Insulin is not, chemically or clinically, a steroid, and its use in non-diabetics is dangerous and always an abuse outside of a well-equipped medical facility.

Inhalable insulin is under investigation, as are several other insulin administration techniques.

There have been attempts to improve upon this mode of administering insulin, as many people find injection inconvenient, awkward, and generally painful.

of quick-acting synthetic insulin following meals containing starchy carbohydrates and protein, but little fat, in an attempt to "force feed" nutrients necessary for growth into skeletal muscle, while preventing growth of adipocytes.

When the glucose level comes down to the usual physiologic value, insulin release from the beta cells slows or stops.

Several other non-transplant methods of automatic insulin delivery are being developed in research labs, but none is close to clinical approval.

Over the spring of 1922, Best managed to improve his techniques to the point where large quantities of insulin could be extracted on demand, but the preparation remained impure.

Insulin is a polypeptide containing two chains of amino acids joined together by two disulfide bridges.

Novo Nordisk has also developed a genetically engineered insulin independently.

Long term risks include development of type II diabetes, and a lifetime dependency on synthetic insulin.

On January 11, 1922, Leonard Thompson, a 14-year-old diabetic who lay dying at the Toronto General Hospital, was given the first injection of insulin.

Rosalyn Sussman Yalow received the 1977 Nobel Prize in Medicine for the development of the radioimmunoassay for insulin.


Low levels of circulating insulin, or its absence, will prevent glucose from entering those cells (eg, in untreated Type 1 diabetes).

The C-peptide of proinsulin (discussed later), however, is very divergent from species to species.

Pulsatile insulin is an additional method of administration of insulin to diabetics.

Choosing insulin type and dosage/timing should be done by an experienced medical professional working with the diabetic patient.

The limitations are cost, the potential for hypoglycemic and hyperglycemic episodes, catheter problems, and no "closed loop" means of controlling insulin delivery based on current blood glucose levels.

Human insulin is now manufactured for widespread clinical use using genetic engineering techniques, which significantly reduces the presence of impurities.

The intended implication would seem to be that insulin has effects similar to those alleged for some steroids.

Insulin production from animal pancreases was widespread for decades, but very few patients today rely on insulin from animal sources.

Endogenous causes of insulin excess (such as an insulinoma) are very rare, and the overwhelming majority of hypoglycemia cases are caused by human action (e.g., iatrogenic, caused by medicine) and are usually accidental.

Improvement in plumbing systems was very slow, with virtually no progress made from the time of the Roman system of aqueducts and lead pipes until the nineteenth century.

Medical preparations of insulin (from the major suppliers—Eli Lilly and Novo Nordisk—or from any other) are never just "insulin in water."

The sympathetic nervous system (via ?2-adrenergic agonists such as norepinephrine) inhibits the release of insulin.

The abuse of exogenous insulin carries with it an attendant risk of hypoglycemic coma and death.

Apart from being the primary agent in carbohydrate homeostasis, insulin in vertebrates has effects on fat metabolism and it changes the liver's activity in storing or releasing glucose and in processing blood lipids.
Insulin from these sources is effective in humans as it is nearly identical to human insulin (three amino acid difference in bovine insulin, one amino acid difference in porcine).

The host cells are then allowed to grow and reproduce normally, and due to the inserted human DNA, they produce actual human insulin.

The exact sequence of amino acids comprising the insulin molecule, the so-called primary structure, was determined by British molecular biologist Frederick Sanger.


When patients were switched from injected to inhaled insulin, no significant difference was found in HbA1c levels over three months.

Other substances known that stimulate insulin release are acetylcholine, released from vagus nerve endings (parasympathetic nervous system); cholecystokinin, released by enteroendocrine cells of Intestinal mucosa; and glucose-dependent insulinotropic peptide (GIP).

Inhaled insulin has similar efficacy to injected insulin, both in terms of controlling glucose levels and blood half-life.

Instead insulin is usually taken as subcutaneous injections by single-use syringes with needles, an insulin pump, or by repeated-use insulin pens with needles.
Both insulin, growth hormone (GH), and insulin-like growth factor 1 (IGF1) are self-administered by those looking to increase muscle mass beyond the scope offered by anabolic steroids alone.

The only inhalable insulin approved by the Food and Drug Administration is Exubera (FDA 2006).

On top of this, non-prescribed insulin is a banned drug at the Olympics and other global competitions.

The Nobel Prize committee in 1923 credited the practical extraction of insulin to a team at the University of Toronto and awarded the Nobel Prize to two men: Frederick Banting and John Macleod.