Facts about Mumps

A research group published a 1996 report on a chemical extracted from Spirulina platensis, a species of blue-green algae, which inhibited Mumps virus in a viral plaque assay (Hayashi et al.

The paramyxovirus that causes mumps is prevalent in the saliva, and is spread from person to person by saliva droplets or direct contact with articles that have been contaminated with infected saliva.

In 1988, it became United Kingdom government policy to introduce mass child mumps vaccination programs with the MMR vaccine, and MMR vaccine is now routinely administered in the UK.

The World Health Organization (WHO) recommends the use of mumps vaccines in all countries with well-functioning childhood vaccination programs.


A University of Tokyo group reported in 1992, that research compound TJ13025 ((6'R)-6'-C-methylneplanocin A) had an antiviral effect on four Mumps virus strains cultured in Vero cells.

The British Medical Association and Royal Pharmaceutical Society of Great Britain had previously recommended against general mumps vaccination, changing that recommendation in 1987.

After adolescence, mumps tends to affect the ovary, causing oophoritis, and the testes, causing orchitis.

The most common preventative measure against mumps is immunization with a mumps vaccine.


Before the introduction of the mumps vaccine, the mumps virus was the leading cause of viral meningoencephalitis in the United States.

The current mumps vaccine used in the United States is a live, attenuated vaccine, the Jeryl-Lynn strain, and was licensed in December of 1967 (Breslow 2002).
Adults infected with mumps are more likely to develop severe symptoms and complications.

The mature testis is particularly susceptible to damage from mumps, which can lead to infertility.

Mumps is caused by a paramyxovirus, which is any virus of the Paramyxoviridae family of the Mononegavirales order.


The mumps vaccine was introduced into the United States in December 1967: since its introduction there has been a steady decrease in the incidence of mumps and mumps virus infection.

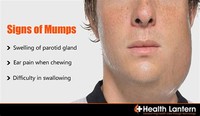
Other symptoms of mumps can include sore face and/or ears, loss of appetite, lack of energy, and occasionally in more serious cases, loss of voice.

Some anti-vaccine activists protest against the administration of a vaccine against mumps, claiming that the attenuated vaccine strain is harmful, and/or that the wild disease is beneficial.
The mumps virus was identified in 1934, and by 1948, a killed virus vaccine was licensed, but later discontinued because of its failure to produce long-lasting immunity (Breslow 2002).

The mumps vaccine used in the United States, which also confers long-lasting immunity, was licensed in December 1967 (Breslow 2002).

The most typical presentation of mumps is painful swelling of the salivary glands (classically the parotid gland) and fever (Enders 1996).

Highly infectious, prior to the development of a vaccine mumps was vary common among children, with most children contracting mumps between the ages of four and seven (Longe 2006).