Facts about Polio

The apparent effects of polio have been known since prehistory; Egyptian paintings and carvings depict otherwise healthy people with withered limbs, and children walking with canes at a young age.
Poliovirus infects human cells by binding to an immunoglobulin-like receptor, CD155 (also known as the poliovirus receptor (PVR)), on the cell surface.

Polio is most infectious between 7–10 days before and 7–10 days after the appearance of symptoms, but transmission is possible as long as the virus remains in the saliva or feces.

The precise mechanism poliovirus uses to enter the host cell has not been firmly established.

Detection of virus in the CSF is diagnostic of paralytic polio, but rarely occurs.

Individuals who are exposed to poliovirus, either through infection or by immunization with polio vaccine, develop immunity.

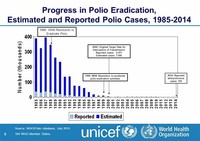
In 1988, a coordinated global effort to eradicate polio, the Global Polio Eradication Initiative, was led by the World Health Organization, UNICEF, and The Rotary Foundation.

Specific strains of each serotype are used to prepare vaccines against polio.

Post-polio syndrome is not an infectious process, and persons experiencing the syndrome do not shed poliovirus.

The Salk vaccine, or inactivated poliovirus vaccine (IPV), is based on poliovirus grown in a type of monkey kidney tissue culture (Vero cell line), which is chemically inactivated with formalin.

Recent experimental evidence supports the latter hypothesis and suggests that poliovirus binds to CD155 and is taken up via endocytosis.

Historically, a noninvasive negative-pressure ventilator, more commonly called an iron lung, was used to artificially maintain respiration during an acute polio infection until a person could breathe independently (generally about one to two weeks).

DNA encoding the RNA genome of poliovirus was introduced into cultured mammalian cells and infectious poliovirus was produced.


Polio victims that develop equinus foot cannot walk properly because they cannot put their heel on the ground.

Many cases of poliomyelitis result in only temporary paralysis.

Infection or vaccination with one serotype of poliovirus does not provide immunity against the other serotypes, and full immunity requires exposure to each serotype.

In 1977, there were 254,000 persons living in the United States who had been paralyzed by polio.

In 1981, Racaniello and Baltimore used recombinant DNA technology to generate the first infectious clone of an animal RNA virus, poliovirus.
The results of a large clinical trial were promising; the gamma globulin was shown to be about 80% effective in preventing the development of paralytic poliomyelitis.
Poliovirus was first isolated in 1909 by Karl Landsteiner and Erwin Popper.

A rare condition with a similar presentation, non-poliovirus poliomyelitis, may result from infections with non-poliovirus enteroviruses.

The mechanisms by which poliovirus spreads to the CNS are poorly understood, but it appears to be primarily a chance event—largely independent of the age, gender, or socioeconomic position of the individual.

Poliovirus can survive and multiply within the blood and lymphatics for long periods of time, sometimes as long as 17 weeks.

In 2000, polio was officially eliminated in 36 Western Pacific countries, including China and Australia.


Before the 20th century, polio infections were rarely seen in infants before six months of age, most cases occurring in children six months to four years of age.

Overall, 5–10% of patients with paralytic polio die due to the paralysis of muscles used for breathing.

The likelihood of developing paralytic polio increases with age, as does the extent of paralysis.

In 2008, the poliovirus species was eliminated from the genus Enterovirus and the three serotypes were assigned to the species Human enterovirus C, in the genus Enterovirus in the family Picornaviridae.

Patients with abortive polio infections (the minor of the two basic patterns) recover completely.

Around a quarter of individuals who survive paralytic polio in childhood develop additional symptoms decades after recovering from the acute infection, notably muscle weakness, extreme fatigue, or paralysis.

Polio had existed for thousands of years quietly as an endemic pathogen until the 1880s, when major epidemics began to occur in Europe; soon after, widespread epidemics appeared in the United States.

Poliovirus is one of the most well-characterized viruses, and has become a useful model system for understanding the biology of RNA viruses.

In 2002, researchers at SUNY Stony Brook succeeded in synthesizing poliovirus from its chemical code, producing the world's first synthetic virus.

Polioviruses were formerly classified as a distinct species belonging to the genus Enterovirus in the family Picornaviridae.

The first close-up photographs of asteroid-like objects were taken in 1971 when the Mariner 9 probe imaged Phobos and Deimos, the two small moons of Mars, which are probably captured asteroids.

Half the patients with spinal polio recover fully; one quarter recover with mild disability and the remaining quarter are left with severe disability.

Small localized paralytic polio epidemics began to appear in Europe and the United States around 1900.
The type species of the genus Enterovirus was changed from Poliovirus to Human enterovirus C.

Nineteen markers were incorporated into the synthesized DNA, so that it could be distinguished from natural poliovirus.

Bulbar polio leads to weakness of muscles innervated by cranial nerves.

Aseptic meningitis (no bacteria) cannot be distinguished clinically from nonparalytic poliomyelitis because of other agents and virus must be detected to confirm diagnosis.

Factors that increase the risk of PPS include the length of time since acute poliovirus infection, the presence of permanent residual impairment after recovery from the acute illness, and both overuse and disuse of neurons.

Individuals who are exposed to the virus, either through infection or by immunization with polio vaccine, develop immunity.

By 1910, much of the world experienced a dramatic increase in polio cases and frequent epidemics became regular events, primarily in cities during the summer months.

The effort to eradicate polio reflects a great spirit of cooperation, creativity, and sacrifice among individuals and organizations.
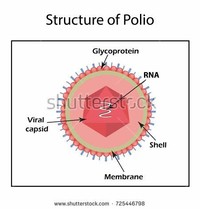
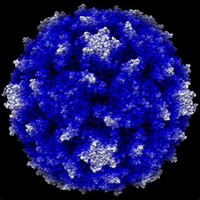
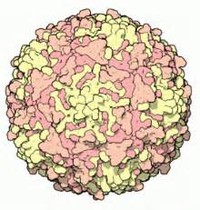
The structure of poliovirus is very simple, composed of a single (+) sense RNA genome enclosed in a protein shell called a capsid.
In 1950, William Hammon at the University of Pittsburgh purified the gamma globulin component of the blood plasma of polio survivors.

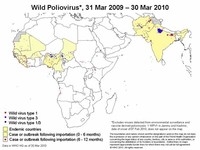
PV1 is highly localized to regions in India, Pakistan, Afghanistan, and Egypt, but following outbreaks of poliomeyletis in 2003–2004 it remains widespread in West and Central Africa.

Fully assembled poliovirus leaves the confines of its host cell 4 to 6 hours following initiation of infection in cultured mammalian cells.


Inactive polio vaccine (IPV) is prepared by formalin inactivation of three wild, virulent reference strains, Mahoney or Brunenders (PV1), MEF-1/Lansing (PV2), and Saukett/Leon (PV3).

The first candidate polio vaccine, based on one serotype of a live but attenuated (weakened) virus, was developed by the virologist Hilary Koprowski.

A single dose of Sabin's oral polio vaccine produces immunity to all three poliovirus serotypes in approximately 50% of recipients.

Bulbar polio often causes death if respiratory support is not provided; with support, its mortality rate ranges from 25 to 75%, depending on the age of the patient.

Other historical treatments for polio include hydrotherapy, electrotherapy, massage and passive motion exercises, and surgical treatments such as tendon lengthening and nerve grafting.
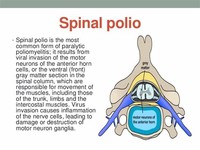
Spinal polio is the most common form, characterized by asymmetric paralysis that most often involves the legs.

The establishment of respiratory centers to assist the most severe polio patients was hence the harbinger of subsequent ICUs.
The World Health Organization estimates that there are up to 20 million polio survivors worldwide.
Today, many polio survivors with permanent respiratory paralysis use modern jacket-type negative-pressure ventilators that are worn over the chest and abdomen.

Maternal antibodies also cross the placenta, providing passive immunity that protects the infant from polio infection during the first few months of life.

Poliovirus enters the body through the mouth, infecting the first cells it comes in contact with—the pharynx (throat) and intestinal mucosa.

Many notebooks are simply bound by a spiral coil at the edge so that pages can be easily torn out.

Both types induce immunity to polio, efficiently blocking person-to-person transmission of wild poliovirus, thereby protecting both individual vaccine recipients and the wider community (so-called herd immunity).
Poliomyelitis is a human infectious disease caused by caused by any of the three serotypes of poliovirus, and spread from person to person, primarily via the fecal-oral route.

Residual complications of paralytic polio often occur following the initial recovery process.

In around 1% of infections, poliovirus spreads along certain nerve fiber pathways, preferentially replicating in and destroying motor neurons within the spinal cord, brain stem, or motor cortex.

Three serotypes of poliovirus have been identified—poliovirus type 1 (PV1), type 2 (PV2), and type 3 (PV3)—each with a slightly different capsid protein.

Developed in the 1950s, polio vaccines are credited with reducing the global number of polio cases per year from many hundreds of thousands to around a thousand.
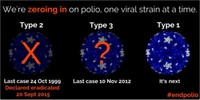
Each of the three known types of poliovirus cause a different form of the disease.

The molecular mechanisms by which poliovirus causes paralytic disease are poorly understood.

After two doses of IPV (given by injection), 90% or more of individuals develop protective antibody to all three serotypes of poliovirus, and at least 99% are immune to poliovirus following three doses.

Hammon proposed that the gamma globulin, which contained antibodies to poliovirus, could be used to halt poliovirus infection, prevent disease, and reduce the severity of disease in other patients who had contracted polio.

The mechanism of viral release from the cell is unclear, but each dying cell can release up to 10,000 polio virions.

Antibodies to poliovirus can be diagnostic, and are generally detected in the blood of infected patients early in the course of infection.

Following the widespread use of poliovirus vaccine in the mid-1950s, the incidence of poliomyelitis declined dramatically in many industrialized countries.

Oral polio vaccine (OPV) contains live attenuated (weakened) strains of the three serotypes of poliovirus.

Accordingly, the rate of paralysis and death due to polio infection also increased during this time.
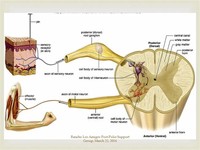
By destroying these nerves this form of polio affects breathing, making it difficult or impossible for the patient to breathe without the support of a ventilator.

Making up about two percent of cases of paralytic polio, bulbar polio occurs when poliovirus invades and destroys nerves within the bulbar region of the brain stem.

Without respiratory support, consequences of poliomyelitis with respiratory involvement include suffocation or pneumonia from aspiration of secretions.

Poliovirus, the causative agent of poliomyelitis, is a human enterovirus and member of the family of Picornaviridae.

Scientists first converted poliovirus's published RNA sequence, 7741 bases long, into a DNA sequence, as DNA was easier to synthesize.

Infection with one serotype of poliovirus does not provide immunity against the other serotypes, however second attacks within the same individual are extremely rare.

Subsequently, Albert Sabin developed another live, oral polio vaccine (OPV).
A laboratory diagnosis is usually made based on recovery of poliovirus from a stool sample or a swab of the pharynx.

Interaction of poliovirus and CD155 facilitates an irreversible conformational change of the viral particle necessary for viral entry.

Poliomyelitis was first recognized as a distinct condition by Jakob Heine in 1840.
Treatment of polio often requires long-term rehabilitation, including physical therapy, braces, corrective shoes and, in some cases, orthopedic surgery.

The neurophysiological processes involved in recovery following acute paralytic poliomyelitis are quite effective; muscles are able to retain normal strength even if half the original motor neurons have been lost.


Polio has also been known as infantile paralysis, since it most commonly infects younger children and could cause of lifetime of paralysis.
Creation of the infectious clone propelled understanding of poliovirus biology, and has become a standard technology used to study many other viruses.

Before the 20th century, polio infections were rarely seen in infants before six months of age, most cases occurring in children six months to four years of age.


Most industrialized countries have switched to IPV, which cannot revert, either as the sole vaccine against poliomyelitis or in combination with oral polio vaccine.

Asymmetric flacid paralysis without sensory loss in a young adult or child, accompanied by a fever, is almost always indicative of polio.

Wild poliovirus type 2 has probably been eradicated; it was last detected in October 1999 in Uttar Pradesh, India.

Three doses of live-attenuated OPV produce protective antibody to all three poliovirus types in more than 95% of recipients.

Poliomyelitis is highly contagious via the oral-oral (oropharyngeal source) and fecal-oral (intestinal source) routes.